
What is a shoulder dislocation?
- Shoulder dislocation occurs when the shoulder joint comes out of the socket (i.e. the humeral head comes out of the glenoid).
- Two main types of shoulder dislocation:
- Traumatic shoulder dislocation
- Atraumatic shoulder dislocation
Traumatic shoulder dislocation
- How does traumatic shoulder dislocation happen?
- It is usually associated with (a) high impact force on the shoulder, e.g. falling on the shoulder / outstretched hand; OR (b) repetitive overuse of the shoulder, resulting in structural damage.
- Examples of structural damage:
- Bankart / SLAP lesion (shoulder joint cartilage tear);
- Hill-Sachs lesion (compression fracture of the shoulder bone);
- Etc.
- How is a traumatic shoulder dislocation diagnosed?
- History of trauma
- Clinical test on shoulder instability
- Imaging, e.g. MRI
- Physiotherapy for traumatic shoulder dislocation
- For younger age patients, patients active in overhead sports and elite competitive athletes, it is recommended that surgical repair of the structural damage is done before commencing physiotherapy, as the risk of re-dislocation is high with conservative treatments alone.
- Patients of older age are recommended to go for conservative treatments, including physiotherapy, first.
- Patients who failed conservative treatments are recommended surgery.
- Physiotherapy processes:
- The physiotherapy processes for both post-op or conservatively-managed patients are similar, except that there may be surgery-specific precautions indicated by the surgeon for post-op patients.
- Phase 1 (Week 1-6):
- Immobilization at a specific shoulder angle with a sling for 1-6 weeks, duration of which depends on patient’s age, the severity of the damage, types of surgery
- Pendulum exercises
- Isometric rotator cuff exercises (for post-op patients, directions of the exercise may depend on the type of surgery)
- Elbow, wrist and hand mobilization exercises
- Phase 2 (Week 6-12):
- Assisted active ranging exercises to regain full shoulder range of motion
- Gradual strengthening of rotator cuff and scapular muscles, according to the available range of motion
- Phase 3 (Week 12 onwards):
- Strengthening
- Power training
- Coordination and agility training
- Assessed for strength and function before returning to sports
Atraumatic shoulder dislocation
- How does atraumatic shoulder dislocation happen?
- Incorrect movement pattern at shoulder joint or scapula
- Shoulder, scapular or even trunk muscles weakness
- General joint laxity
- Persistent shoulder muscle cramp leading to muscle imbalance
- Nerve disturbance / damage
- Previous minor shoulder trauma without structural damage, but resulting in muscle switching off / muscle cramp as a protective mechanism
- How is an atraumatic shoulder dislocation diagnosed?
- History – Any trauma, what movements trigger/ease the dislocation
- Clinical test – on shoulder instability, muscles activation, nerve disturbance if any
- Imaging as necessary to rule out any structural damage
- Physiotherapy for atraumatic shoulder dislocation
- No one-size-fits-all protocol as the root causes are different across patients with asymptomatic shoulder dislocation
- To tackle muscle weakness: targeted strengthening exercises
- To tackle muscles that are switched off: facilitated correct movement, verbal/visual / tactile cues
- To tackle nerve disturbance: identify the cause of disturbance e.g.compression by neck/shoulder structures, and treat accordingly. May refer to doctor for medication as necessary
- Patients with atraumatic shoulder dislocation may need a combination of treatments if their dislocation involves more than one factor.
Reference:
- Drummond JM, Popchak A, Wilson K, Kane G, Lin A. Criteria-based return-to-sport testing is associated with lower recurrence rates following arthroscopic Bankart repair. J Shoulder Elbow Surg 2021; 30:S14–S20
- Barrett C. The clinical physiotherapy assessment of non-traumatic shoulder instability. Shoulder & Elbow 2015; Vol. 7(1): 60–71
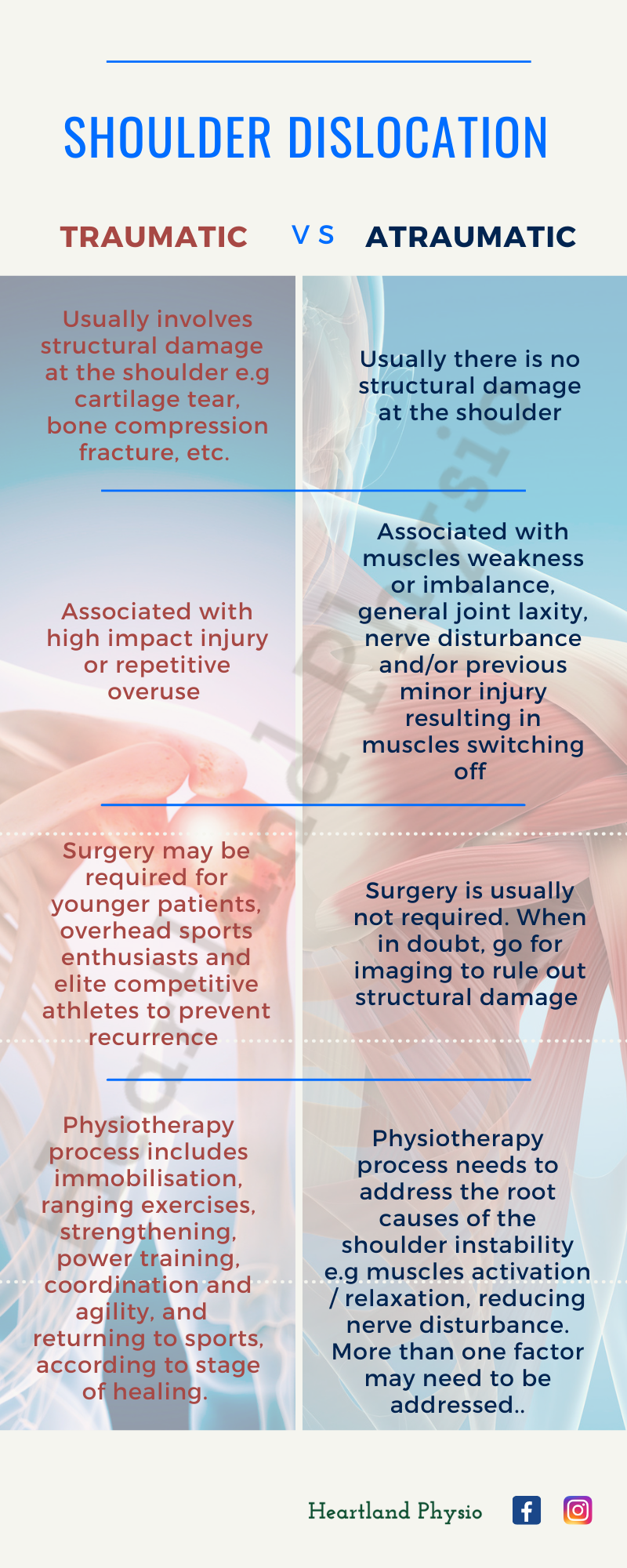
Shoulder Dislocation Infographic:
A quick recap on the 2 main types of shoulder dislocation and their physiotherapy management.